
Generic substitution: a map of the influences affecting the pharmacists’ decision process
In recent years, more and more attention has been paid to the effects of generic substitution. Preferred supplier contracts (“preferentiebeleid”) are a known cause for generic substitution. However, a recent study has shown that the majority of substitutions are towards a non-preferred drug (a total of 77% of all substitutions), and for these substitutions the direct cause is unknown. The various participants in the pharmaceutical chain all appear to influence the choice of generic brand by the pharmacist.
In this study, commissioned by the Department of Medicines and Medical Technology of the Ministry of Health, Welfare and Sport (“VWS”), we assess the relative strength of influence from various participants in the pharmaceutical chain that may cause substitution to a non-preferred generic drug.
The final choice for a particular brand, and therefore also the choice to substitute, takes place at the pharmacists’ counter. There are five factors the pharmacist takes into account in the choice of brand, arising from its two roles:
- Providing care. A pharmacist aims to provide high-quality pharmaceutical care. This means the pharmacist includes the following criteria as he chooses a brand:
- Quality of care
- Client satisfaction
- Operating a business. In addition, the pharmacist makes considerations appropriate to running a healthy business. This means the pharmacist also incorporates the following criteria in its decision process:
- Reimbursement
- Purchasing power
- Operational excellence
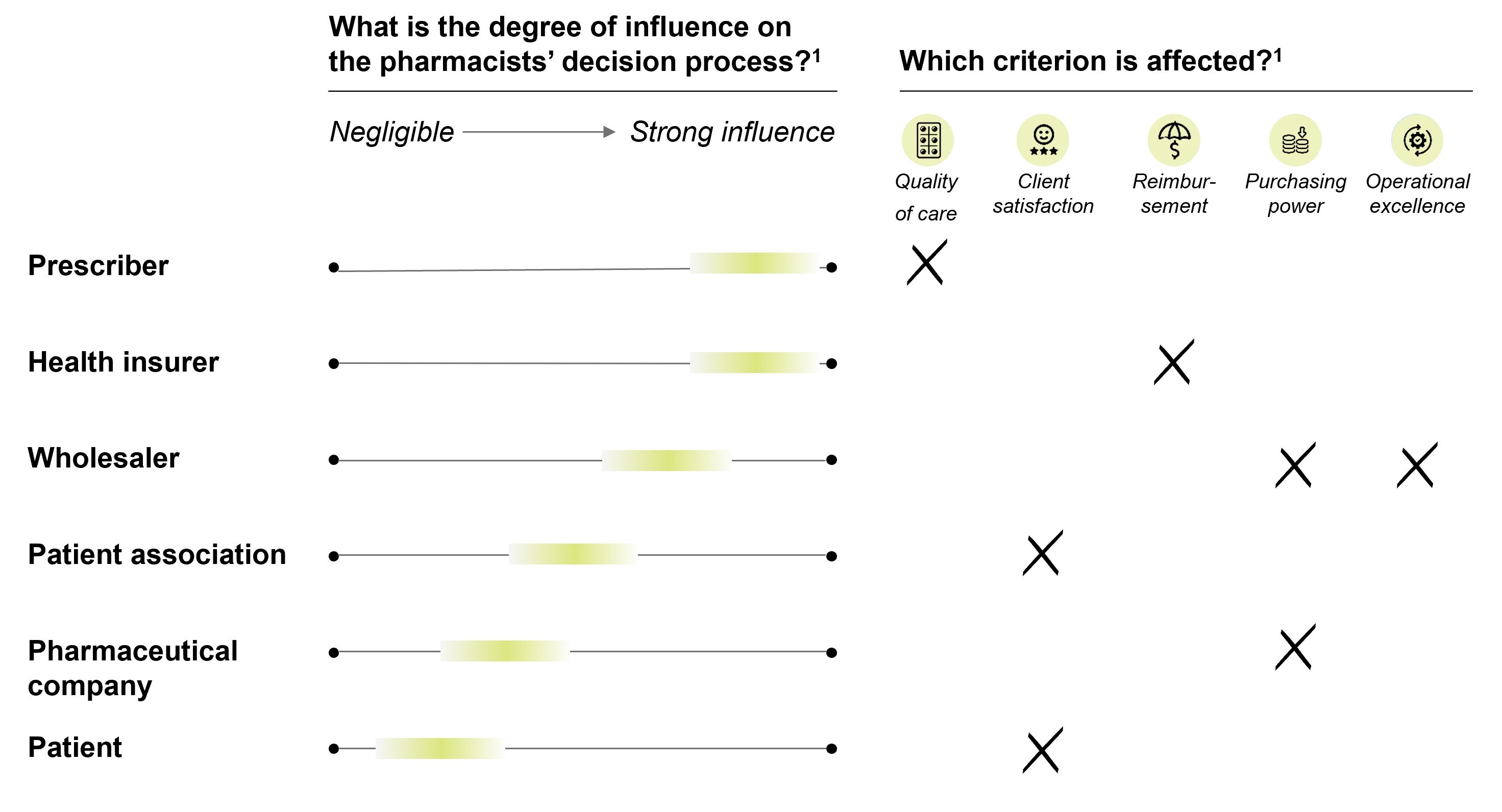
In varying degrees, all participants in the pharmaceutical chain influence the pharmacists’ decision process. The strongest influence comes from prescribers and from health insurers. The prescriber primarily affects the criterion ‘quality of pharmaceutical care’, while health insurers influence the criterion ‘reimbursement’. Although not quite to the same extent, wholesalers also have a strong influence on the pharmacists’ decision process. The wholesaler influences the criterion ‘purchasing power’ and ‘operational excellence’ through its own preferred supplier process, knows as a purchase mandate (in which the pharmacist provides the wholesaler a mandate to close preferred contracts on its behalf), operational and IT support and access to benefits such as centralized parallel import. All of these influences can potentially lead to drug changes. Although the different stakeholders all influence the pharmacists’ decision process, the interplay of the various incentives within the unique context of the pharmacist can vary considerably.
Based on our research, we conclude that in the first place it is important to alleviate the perceived negative impact of generic substitution. To this end, we see four solutions, ordered by increasing gravity of the intervention:
- Reduce the negative perception of generic substitution by improving and standardizing the guidance and communication to individual patients, and/or conducting a public campaign
- Offer a platform within the Personal Health Environment (i.e. “Persoonlijke gezondheidsomgeving (PGO)”) where patients can voice their concerns and experiences
- Offer patients more freedom of choice in exchange for a greater private contribution to the associated additional costs
- Standardize packaging and contents
As generic substitution is primarily the result of incentives within the pharmaceutical chain to control pharmaceutical costs, solutions to reduce the number of substitutions are likely to increase costs. That being said, ways to reduce the number of substitutions are of course conceivable. For example:
- Intervene in purchasing policies of health insures (for example: contracting multiple preferred suppliers within each cluster)
- Intervene in purchasing policy of wholesalers (for example: drafting, publishing and acting upon a code of conduct regarding the contracting of preferred suppliers)
Although even more radical, it is also possible to change the health care system itself. For example:
- Draft a guideline recording the maximum number of drug changes per patient in a certain period
- Assign the procurement role completely to the government
- Assign the procurement role completely to the health care insurers
- Assign the procurement role completely to the wholesalers and pharmacies